
 Admin_Adham
Admin_Adham
After all the headlines about “Ozempic mouth” — and “Ozempic breath” and “Ozempic teeth” — emerging research points to possible explanations, notably how GLP-1 drugs delay the emptying of the stomach and intestines.
When the CEO of Hershey recently credited GLP-1 users with a spike in sales of sugar-free mints and gum, the drug’s oral-related effects got the attention that dentists had already noted. But as more patients taking GLP-1 report oral changes, reflected in a nascent but growing body of literature, questions arise for clinicians about how to manage them. And halitosis is far from the only issue.
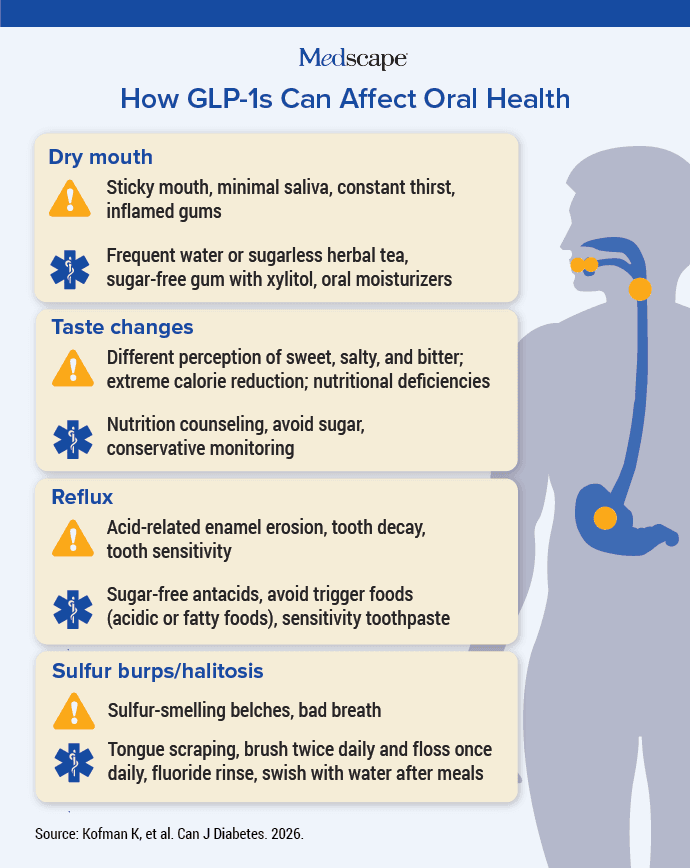
Dry mouth, or xerostomia, is the most common oral change, said Jennifer L. Thompson, DDS, chair of the American Dental Association Council on Dental Practice. That “can contribute to other challenges like bad breath, changes in taste such as a metallic or bitter sensation, tooth sensitivity, and an increased risk of cavities and gum disease.”
Up to 24% of users report vomiting, which brings harsh stomach acids into the mouth. This can lead to tooth decay and bad breath. Some research suggests that gastrointestinal adverse effects and dry mouth occur more often with semaglutide (Ozempic and Wegovy) than with other GLP-1 receptor agonists.
Research Points to Delayed Gastric Emptying
Most of these oral symptoms are a downstream result of delayed gastric emptying, said Aviv Ouanounou, DDS, an associate professor at the University of Toronto Faculty of Dentistry in Toronto, Ontario, Canada. He’s the co-author of a forthcoming paper (now in preprint) on the possible oral health effects of semaglutide.
GLP-1 therapy “can lead to prolonged retention in the stomach, in the intestines,” Ouanounou said. “That creates an environment which is a conducive to bacterial overgrowth, to fermentation, causing odor perceived as bad breath.” This can lead to a buildup of hydrogen sulfide, causing so-called sulfur burps.
Another in-press paper, published online this week, analyzed International Classification of Diseases codes from records of more than 200,000 GLP-1 users and found patients were 32.9% more likely to experience gastroesophageal reflux disease. Reflux and regurgitation can cause more bad odor and erosion of the enamel, Ouanounou said. (That study found no link to bad breath or dry mouth, though these symptoms may have been left out if they weren’t recorded by a diagnosis code.)
“Studies are limited with direct links to GLP-1s,” Ouanounou said, “but the mechanism, the pathways of the slow motility, leads to all these things, consistent with GI [gastrointestinal] physiology.”
Dry mouth might be a direct effect. A recent review of studies on the mechanism of oral effects found that the drugs may interact with the salivary glands — again, semaglutide more than others. Saliva production depends on a delicate back-and-forth between calcium and cyclic adenosine monophosphate signals inside salivary gland cells. If semaglutide keeps the GLP-1 receptor active for too long, it may throw off that balance, reducing secretion and desensitizing the glands over time.
“Saliva plays an especially important role in protecting teeth by washing away food and neutralizing acids produced by plaque,” Thompson said. “When saliva is reduced, these bacteria can grow more easily, increasing the risk of tooth decay, gum inflammation, and bad breath.”
As for changes in taste perception, the relationship has yet to be clearly defined. But the naturally occurring peptide hormone GLP-1 is involved in taste mechanisms. A 2026 review of literature found that in the taste buds, it seems to make certain flavors less noticeable by changing how taste cells respond and how they send signals. In the brain, GLP-1 activity appears to reduce the reward response to sweet foods and may make bitter tastes feel more unpleasant.
Not enough evidence exists yet to know whether oral changes in an otherwise healthy GLP-1 user could indicate a more serious problem. Even so, they shouldn’t be ignored.
“Oral changes alone do not diagnose gastroparesis, SIBO [small intestinal bacterial overgrowth], or another gastrointestinal condition,” Thompson said. “However, persistent or worsening oral symptoms, especially when paired with gastrointestinal symptoms, may prompt further discussion.”
Helping Patients Manage the Symptoms
While dry mouth and sulfur burps might not be reason enough for a patient to discontinue the use of a life-changing drug, nobody enjoys the experience. Good oral hygiene — twice-daily brushing for 2 minutes each time and flossing at least once a day — can help, as can these other measures recommended by the American Dental Association and/or Ouanounou:
Dry Mouth
- Advise patients to drink plenty of water or herbal tea without sugar.
- Stimulate saliva production with sugar-free gum or pastilles containing xylitol, a sugar alcohol shown to prevent tooth decay. The act of chewing gum itself increases saliva production.
- Recommend over-the-counter oral moisturizing rinses, sprays, gels, or lozenges.
- In severe cases, consider prescribing pilocarpine to boost saliva production.
Changes in Taste Perception
- Suggest smaller, more frequent meals to better tolerate the effects.
- Refer patient for nutritional counseling to maintain a balanced diet.
- Monitor the patient closely because altered taste perception can lead quickly to nutritional deficiencies.
Reflux and Vomiting
- Encourage patients to replenish fluids consistently and eat smaller, more frequent meals.
- Suggest sugar-free antacids.
- Help patients identify trigger foods or behaviors to avoid — they might include certain acidic or fatty foods or smoking.
- Advise against brushing teeth right after vomiting when tooth enamel is softened and vulnerable to mineral loss. Instead, have them swish with water immediately and wait at least 30 minutes to brush.
- Recommend using toothpaste formulated for sensitive teeth.
- Consider modifying the medication dose to reduce vomiting.
Sulfur Burps and Halitosis
- Advise the use of a fluoride-containing antibacterial toothpaste, preferably with zinc, to help neutralize sulfur compounds and kill odor-causing bacteria.
- Recommend tongue scraping and flossing at least once a day.
- Instruct patient to swish and spit out water after eating to remove food debris.
- Recommend a fluoride-containing mouth rinse.
Conditions such as dry mouth, vomiting, and reflux put a patient at a higher risk for tooth decay. If they’re not able to follow recommendations — or if the suggestions don’t help their symptoms — encourage them to see their dentist every 3 or 4 months rather than the standard 6-month interval.
The experts cited in this article reported no relevant disclosures.

